
The Rh blood group system is spectacularly complex, while at the same time enormously important. Beginners trying to understand the system are often really confused by all the terminology that blood bankers use to describe the five main Rh antigens. We say things like, “well, the most likely genotype is R1R1, obviously” when it just isn’t obvious at all when you are trying to figure things out! Further, the genetics of this system have been variously understood and explained over the years, and it is very easy to get lost in the jungle of phrases and haplotypes and buzzwords!
“But, Joe,” you cry, “surely you can make this easy for us!” My friends, the answer is “no, I’m just not THAT good (and don’t call me “Shirley”)! But, I can make it easier!” This post is designed to help you get started on the right track, and is the first of two on this topic.

The Rh blood group system is a complex set of red blood cell surface proteins that most likely function to maintain the integrity of the cell membrane. As of May 2016, we know of at least fifty Rh antigens according to the International Society for Blood Transfusion, but we spend most of our time worrying about only five of them. Those five (which we call “D, C, c, E, and e”) account for the vast majority of clinical and laboratory issues in this blood group, and for most of the confusion that people learning the terminology experience!
The Deal with D and d
Before we get rolling, you must understand this: The D antigen is the main Rh antigen. The presence or absence of D defines a person as “Rh positive” or “Rh negative,” an extremely important distinction that establishes a person’s basic blood type (in conjunction with their ABO type). Commonly, blood bankers will use the term “d” (“little d”) to indicate the lack of the D antigen (in other words, we will describe someone who is Rh negative either as “D-negative” or when writing it, as “d”). Little d is a silly way to say or write it, because there is no little d antigen; little d is merely a slang term to indicate that there is no D.
Ancient History
Years ago, based on the theories of Fisher and Race in England, blood bankers believed that the five main antigens were inherited as a combination of alleles from three different genes: One D gene, one gene for C or c (called “C/c” which coded for either C or c, not both), and one gene for E or e (called “E/e” and likewise coding for either E or e). Each child received a group of Rh genes from each parent (a so-called “haplotype“), and the combination of alleles inherited from both parents resulted in the child’s final Rh phenotype. We now know that this theory was wrong (more on this in a minute), but the names for the five main antigens (D, C, c, E, and e) stuck around.
Meanwhile, another famous blood banker, Dr. Alexander Wiener, was developing his own theory and shorthand terminology scheme. Most of what he proposed has been discredited, but he did develop something that we still use today. Dr. Wiener gave shorthand names to the eight possible haplotypes resulting from the possible combinations of the alleles of those three genes mentioned above. Those names are blood bank gospel, and you must memorize them if you are going to be involved in blood banking! Plus, virtually anyone writing test questions covering the Rh system will expect you to know them cold! Here is the modified Wiener terminology for the eight Rh haplotypes:
| D-positive Haplotypes | D-negative Haplotypes |
|---|---|
| R1: DCe | r': dCe |
| R2: DcE | r": dcE |
| R0: Dce | r: dce |
| Rz: DCE | ry: dCE |
Looks Complicated! How Do I Memorize This?
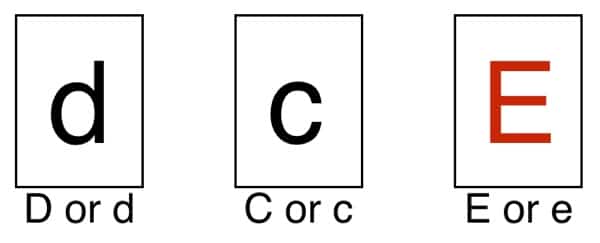
Don’t worry; I’m not going to stop there! There are ways to break this down to make it more manageable. First, look closely at the table above and notice that all the D-positive combinations (haplotypes) in the left column have the a capital “R” as the letter in the shorthand (and start off with a capital “D” in the list of three antigens). Conversely, it’s easy to see that all of the haplotype that start with a small “r” lack D (remember, all of these have a “little d” at the start of the list of three antigens in the haplotype, but there is no “d,” only the absence of “D”). So, the main part of your work is already done! You know that any haplotype that starts with “R” has a “D,” and any that starts with an “r” does not have D (so you write that as “d”). You just have to figure out the combination of C/c and E/e that makes up the rest of the list of three antigens in the haplotype. Look at the image below: You’ve already completed the D/d position by looking at the haplotype. You’ve got two positions left to fill (the C/c and E/e positions):
Good news! The number, letter, or symbol after the “R” or “r” guides you on how to fill in the boxes above. Here’s how to do it:
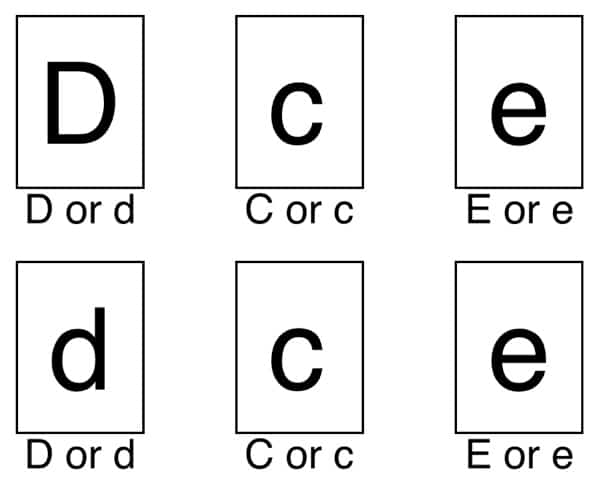
Rule 1: The number 1 or ‘ (single prime) after the R or r, respectively, tells you to capitalize the first of the two remaining openings, the C/c position, and results in a “Ce” combination.
For example, for R1, the first position, C/c, is capitalized and the second, E/e, is not, like so:
R1 Haplotype
The same rule applies to r’, but the haplotype lacks D (written as “d”):
r’ Haplotype
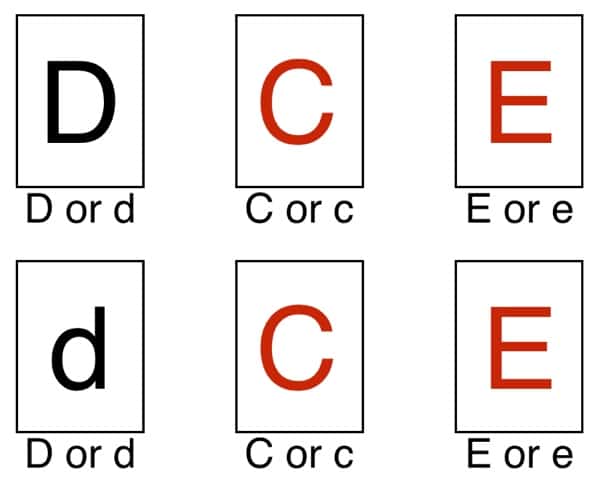
Rule 2: The number 2 or ” (double prime) after the R or r, respectively, tells you to capitalize the second open position, the E/e, and results in a “cE” combination.
For example, for R2, the second position, E/e, is capitalized and the first, C/c, is not, like so:
R2 Haplotype
Obviously, the same rule applies to r”, but this haplotype also lacks D:
r” Haplotype
Rule 3: 0 or nothing after the R or r, respectively, tells you that neither of the two open positions is capitalized, and results in a “ce” combination.
Hopefully, this is becoming obvious, so the image below shows both R0 (on top) and r (below):
R0 (top) and r (bottom) Haplotypes
OK, here’s a weird little tidbit: If you look at the “0” in the R0 haplotype, you will notice that it looks like a “zero” rather than the letter “O,” right? It’s usually written that way (it definitely is in the AABB Technical Manual), but blood bankers always say it like the letter O. In other words, you would pronounce “R0” as “R Oh” rather than “R zero.” Blood bankers do weird stuff…
Rule 4: Any letter after the R or r tells you that both of the two open positions are capitalized, and results in a “CE” combination.
Here are Rz and ry:
Rz (top) and ry Haplotypes
Memorize That, But Here’s Reality
After years of further research, it is now clear that these five antigens are the result of the actions of two genes on chromosome 1 rather than three (Update: This was brilliantly and correctly proposed by Dr. Patricia Tippett, as kindly pointed out in the comment section below by Malcolm Needs). As was thought before, the D antigen actually is the product of the actions of a single gene, but that gene is now known as RHD. On the other hand, instead of a single gene controlling expression of C/c antigens and another gene regulating E/e antigens, both sets of antigens are derived from the actions of a separate, single gene, known as RHCE. The four main alleles of the RHCE gene are RHCE*ce, RHCE*cE, RHCE*Ce, and RHCE*CE (Note that sometimes people will write “RHCE*ce,” for example, as “RHce.” It’s shorter and simpler, and while not perfectly correct, people know what you mean. I will do that in some of the rest of this post). Each parent contributes one RHD and one RHCE allele to make up a child’s Rh type (expressed as the presence or absence of the main five Rh antigens above). While the old theories were wrong, the basic idea of haplotypes is still ok to use, as the RHD and RHCE alleles do tend to be inherited as a group (in other words, they are “linked” and it is reasonable to consider them as one group).
NOTE: This terminology can be confusing, especially with RHCE. Remember, the gene is known as RHCE, but that doesn’t mean that all RHCE genes encode C and E antigens. Rather, four possible alleles (alternate forms of the gene) can occur at the RHCE locus on chromosome 1. Only one of those alleles is inherited from each parent. For example, a person could inherit an RHCE*Ce allele at the RHCE gene site. See the table below.
| RHD Gene Possibilities | RHCE Gene Possibilities |
|---|---|
| RHD allele | RHce allele |
| Deleted RHD allele | RHcE allele |
| Mutated RHD allele | RHCe allele |
| RHCE allele |
| D-positive Haplotypes | D-negative Haplotypes |
|---|---|
| R1: RHD + RHCe alleles (DCe) | r': Absent/mutated RHD + RHCe alleles (dCe) |
| R2: RHD + RHcE alleles (DcE) | r": Absent/mutated RHD + RHcE alleles (dcE) |
| R0: RHD + RHce alleles (Dce) | r: Absent/mutated RHD + RHce alleles (dce) |
| Rz: RHD + RHCE alleles (DCE) | ry: Absent/mutated RHD + RHCE alleles (dCE) |
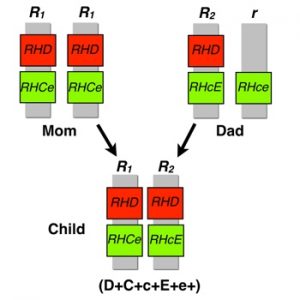
Note that each child inherits only one copy of chromosome 1 from each parent. In the example above, the child received the R1 from mom, and the R2 from dad. The child’s final Rh phenotype is determined by the combination of genes he received from his parents. Note that the alleles are “codominant,” meaning that all of the inherited alleles lead to expression of the coded antigens. In this case, all C/c/E/e combinations are expressed (in other words, if a person has one RHCe and one RHcE allele, all four antigens are expressed). This is shown in the simple Punnett square below showing the genotypes and phenotypes of the offspring of an R1R0 parent and an rr parent:
| R1 (RHD, RHCe) | R0 (RHD, RHce) |
|
| r (“RHd”, RHce) | R1r (D+C+c+E-e+) | R0r (D+C-c+E-e+) |
| r (“RHd”, RHce) | R1r (D+C+c+E-e+) | R0r (D+C-c+E-e+) |
| Haplotype | Caucasians | African-Americans | Asians |
|---|---|---|---|
| R1 | 42% | 17% | 70% |
| R2 | 14% | 11% | 21% |
| R0 | 4% | 44% | 3% |
| Rz | <0.01% | <0.01% | 1% |
| r' | 2% | 2% | 2% |
| r" | 1% | <0.01% | <0.01% |
| r | 37% | 26% | 3% |
| ry | <0.01% | <0.01% | <0.01% |
As you would expect from the presence of two genes in the Rh system, two separate proteins carry these Rh antigens, with one protein (called “RHD”) carrying D and another (called “RHCE”) carrying the combination of C/c and E/e (as well as the rest of the Rh antigens outside of the first five). The proteins are very similar in appearance (and likely, in function), and both appear to be dependent on the presence of another protein known as “Rh-related Antigen” (or “RhAG”) for expression.
So, What Now?
If this is your first exposure to this stuff, take a little while and make sure that you can generate the list of the 8 possible haplotype designations. As I mentioned, it is crucial that you know them. You should also learn at least the two most common Rh haplotypes in each race listed on the table above. In a future post, I will outline how we can actually use those combinations to solve problems, and how they are assessed commonly on examinations.
If this post looks familiar to long-time BBGuy.org readers, it’s because it is a heavily modified and (hopefully) clarified version of a post from 2011.











Brilliant, as ever. Just a couple of things. It would, perhaps, have been nice to mention the fact that the two gene theory was first put forward by Dr Patricia Tippett, who is still well and as sharp as a needle, despite having retired many years ago now. I have a recent photograph of her, but cannot attach it here. I will email it to you, if you could provide an email address.
The other thing is, and I may be completely wrong here, I always thought that, when the nomenclature RHCE*ce (I know, it should be italicised, but I can’t do it here!) is used, the “*” meant that the genotype had actually been “proved” by molecular techniques, rather than just by serological techniques. As I say, I may be wrong – it wouldn’t be the first time, and I have very grave doubts that it will not be the last time!
Malcolm, thanks for the reminder about Dr. Tippett. You are right; she deserves mention, and I have updated the post to reflect that. As for the nomenclature stuff, honestly, I’m not remotely a geneticist, and the details of that issue go far more into “the deep end of the pool” than is necessary for this post, I think. I’m sure that you are right; I defer to your expertise, but don’t think it will matter to most people learning about this! Thanks, as always, for your kind comments.
I was struggling with this same thing until I read this comment. You cleared it up for me, thank you!
thank u very much please we need a video about SCT
Thank you so so so much!
Finally got it.
May GOD bless you!
Can you tell me what B Rh Pos c D Ě means? I had to get a jag after giving birth
Hi! I’ve been studying for the exam and your website is very helpful.
On the table showing the offspring’s phenotype and genotype, if R1 was inherited , there shouldn’t be an “E” ?
Remember, the “R1” haplotype designation means that the person has inherited two alleles: RHD and RHCe. That means that combination gives a D antigen, a C antigen, and an e antigen (NOT an E). I think that the table you are referring to shows the possibilities with an R1R0 and an rr combination. None of those haplotypes would impart an E antigen. I hope that makes sense! Joe
Joe. I know it’s a couple years late but the table showing the haplotypes with an R1R0 and an rr combination actually shows an E antigen in all four offspring, as well as a C antigen for the R0r offspring. I believe that is what lavender1216 was trying to ask.
BTW…love this site!!
I don’t THINK the table shows that, Jay! There is a “-” after the E in all four places, and for R0r, the C also has a “-” after it, indicating the LACK of that antigen.
-Joe
After 25 years of working in my lab, and only performing the most basic of blood banking, the powers that be want the staff to start performing panels. Yikes! Your site has helped me refresh those long ago forgotten techniques. Thanks for being there!
Kitty, I’m glad to be of help to you! What you are describing is not uncommon in U.S. labs today, as fewer and fewer qualified staff are available, it seems. I wish you the best as you navigate tricky waters. The content on this site, in part, is designed for people like you who are learning (or re-learning in your case) the field.
Joe
I have a child who has liver cancer and has been old she has blood that can not be typed because it reacts as all known types. I am trying to understand how is this possible? They cant type her blood by standard tests.
Carlene, I’m so sorry to read about your child’s liver cancer. Unfortunately, there is no way to evaluate your situation without more information, and I can’t do internet consultations. Please talk to local transfusion medicine experts in your area! Most every hospital can find someone who has enough experience and knowledge to discuss your child’s case intelligently (often, that will be the doctor overseeing your blood supplier, but in some hospitals, the expert may actually already work there). I wish you and your family the very best.
-Joe
I am currently preparing for my ASCP exam. I just want you to know how grateful I am for your site. It is very helpful. Everyone in my review class checks out your blogs and videos. You are one famous guy in our class ! Thank you sooooooooo much again xo
Thanks, Vanessa! That’s very nice of you to say. I’m happy to help.
-Joe
These are very detailed and interesting information. I’m a medical laboratory science student and these information helped a lot, thank you very much .
I was understanding fine after reading this blog..and then I come across this question:
The Wiener nomenclature for the E antigen is:
A. hr´
B. hrv´
C. rh˝
D. Rh0
Lost again.. Please help..where did the little “rh” and “hr”s come from?! UGH!
Sincerely,
Frustrated Student
Don’t be frustrated! You have run across some very archaic terminology; in fact, the question is asking you to know Wiener’s names for the five Rh antigens. As the post mentioned, The names for the five main Rh antigens in the Fisher-Race terminology are D, C, E, c, and e. Wiener called them something different (and a LOT more confusing!). Here’s how they correspond:
Fortunately, those terms are rarely used any more, as pretty much everyone uses the Fisher-Race, or “DCE” terminology. Wiener’s original names only appear in old articles, conversations with blood bankers who have been around for a long time, and occasionally, on exams and practice exams, as it seems you have experienced! You can clearly see the pattern above (rh means a capital C or E while hr means a small c or e; ‘ means C or c, ” means E or e), so it shouldn’t be terrible to spend a minute to remember these before an exam. In real life, though, you will rarely see or hear them!
-Joe
thanks joe
Thanks so much Joe, I had this come up at the end of a review assignment and I had never seen it. Not in my work, not in textbooks, not in PowerPoints. Even Google failed to figure out what any of these terms related to, often ignoring any of the ‘ or ” symbols included in the search and defaulting to Anti-Rh = Anti-D
I figured it had something to do with the Wiener nomenclature but its nice to finally see some confirmation on those Anti-hr ones.
thanks for your great explanation. can i use this for my students? thank you again
Of course! This site is designed to be a help to those teaching blood banking and transfusion medicine. I only ask that you attribute appropriately and avoid changing my words.
-Joe
I was told once I had 0+ with a genotype of r2r2 (not R2R2) and rare. I was reading this article to try to figure this out, but over my knowledge base here and not really understanding in laymen’s terms.
Jennifer, send me an email through the comment page and I’ll be happy to try to help. I can’t do medical consultation over the internet, of course, but I’ll do what I can. Thanks for writing!
-Joe
I got it! I was struggling for days to memorize the Rh nomenclature and now I have a good grasp of this material. I am preparing to take my MT certification next week and this is just helpful. Thank you.
I’m so glad to help you, Judy! Best of luck on your exam!
-Joe
Hi,
I am 52 years and old and 15 years ago I delivered my son 5 weeks early due to escalating antibodies. Post delivery (my son with bad jaundice, but otherwise healthy) the below information was explained to me by the hospital’s hematologist. He said my blood combination was rare. I have since been diagnosed with an autoimmune disorder – rheumatologist says my tests look like I have Lupus, but I’ve had no symptoms in the 13 years since it was discovered after my delivery.
Anti C
Anti c
Anti E
I was told I need:
c-E blood
Question, is this blood difficult to find? Should I be stocking up on my own blood, God forbid, I ever need it? Should my two children be tested for similar blood related issues?
Many thanks,
Heather
Heather, thanks for reading the blog and for your question. Unfortunately, there’s a decent amount of detail in the response, and I can’t give you medical advice through this site. Here’s what I can say: Anyone with antibodies in their blood against what we call “antigens” on red blood cells that are not in the ABO system and the main Rh antigen (we call that one “D”) should clearly understand what that means to them and their future possible transfusion needs. The only way to do that, in my view, is to have a conversation with someone who can be involved in your care, such as a personal physician. Now, you may have to be persistent with this, as it’s very possible that those antibodies may have gotten weaker (or even disappeared over time), so your testing may appear different now than it did 15 years ago. Also, many healthcare providers don’t have a lot of experience dealing with these types of antibodies, and it may require a discussion with a hematologist or Transfusion Medicine specialist at the hospital where you were tested before to sort it all out. In the end, though, you should have someone review the exact antibodies you had then and have now, and be able to understand exactly what it means. I encourage you to be persistent. If worse comes to worse, your local blood donor center will generally have a physician overseeing things that you could discuss this issue with. I wish you the best.
-Joe
thank you so much for clearing this up!! i am now enrolled in an SBB program and this helped ALOT! will be visited this blog and your others to help clear the murky waters i’m in now!
Hello, I donated blood today and the nurse put a sticker on the bag to say it was suitable for neonatal babies. I’m O+ and apparently R1R1 – she said look it up on the internet – which I have done and found you – but nothing I have read tells me why my blood is suitable for newborn babies. I’d love to know why – just curious. TBH I don’t care who gets my blood as long as it helps them.
Hi Nada! Sorry it took me awhile to respond. I can’t say for sure why the nurse said that, but it is most likely due to the combination of you being blood group O (which means your blood can go to any other blood type: A, B, or AB, as well as others that are group O) and being negative for a virus called “cytomegalovirus (CMV).” Again, I can’t say that for sure, but that is most likely. CMV is a big deal for little babies, so we try to give them blood that is less likely to give them that infection. By the way, since you are O positive instead of O negative, your blood might not be used for all babies, but it would certainly be useful for babies who are Rh positive like you. Most importantly, thank you so much for donating! We need blood every day, and I’m sure your donation will be used in the best possible way.
-Joe
I have a card from the hospital over 35 years ago saying I am A r’r blood group. I was told it is rare that I cannot give blood as I had anti D after giving birth.
Is this blood group correct as I cannot see anything on line
Susan, this response will not be adequate at all, but here’s a quick attempt:
For more information, you should speak to a local blood bank director in a hospital or blood center near you. Only they could speak more directly to your circumstances. I wish you the best!
-Joe
I had anti-D and am a blood donor in the UK so women who want to donate blood, but have assumed they can’t, check it out with your local donation organisation.
I am an Rh negative UK female donor.
I think there may be a confusion here between women who have developed antibodies to the RhD antigen and us women who have had a jab against developing such antibodies.
Having anti-D antibodies means can’t continue to donate, (e.g.,https://nibts.hscni.net/spotlight-christinas-story/) whereas having anti-D jab/s (RhoGAMin US), to prevent the formation of antibodies, can donate.
I love you sir !!! I can’t tell you how helpful it was.You are a savage.I watched alot of videos but still got nothing and this explaination just solved everything.It was my 1st time on your website but it won’t be the last time I believe.
i was just going through Rh blood group system and find ur blog sir…this was really very helpful..thanks for explaining beautifully.good enuff to memorize now.
will read more of your blogs.keep it up…
Why RH system show dosage effect as my one senior they show one say they don’t show how to explain them
Sei un genio!
Excellent work Joe. I find all the information here really handy and informative.
Keep up the good work.
Regards
Gurbaksh
We had genotyping done on a WAIHA who’s Rh Control and Anti-D were both 4+ (invalid!). Genotype we were given is RHCE*cd, RHCE*cE ….. does this give us answer to wether he is Rh Positive or Negative?
Unfortunately, it appears there’s a typo in that genotype, Sharon! I’m not familiar with “RHCE*cd” and I asked a good friend who is an Rh genetics expert as well, and that person feels the same. It seems more likely that was intended to be “RHCE*ce” which would mean the answer to your question is that those results do NOT tell you whether the person is D-positive, D-negative, or has a D variant. You need specific genetic testing on the RHD gene to get that answer. The results you have quoted are for the OTHER Rh gene, RHCE.
-Joe
Hi Joe,
I’m a medical laboratory student and as much as I have a passion for blood banking and transfusion science, sometimes the content can get a little tricky! But your site has definitely helped me navigate me through any concerns I have had. Thanks so much for your dedication for teaching! It is obviously doing so many people a lot of good.
Danni
I’m honored that you feel that way, Danni, and grateful that you took the time to write. Best wishes in your studies!
-Joe
Thank you so much for taking the time to explain this in such an easy-to-understand way! As a biochemist currently doing some background training in the transfusion lab, your blog has been an absolute lifesaver whilst navigating this new field!
Vala, you are most welcome. I’m honored to help you!
-Joe
Thanks for your informative post,
this made my immunohaematology lectures for MLT students much much more easier to understand…
THANK YOU SO MUCH. This has really helped me break down how to remember Fisher-Race Terminology!
Could you please explain how a sickle protocol unit of blood is negative for little e?
Not quite sure what you are asking me, Sandy. Please send me a direct email by using BBGuy.org/ask, and I’ll try to help if I can.
-Joe
hey Joe,
Interesting read. I am curious if you could help me understand something. “A Little Back Story.” I have known I was A+ since my first child in 1991 but in 2007 I was in a car accident and lost a lot of blood so I had to receive blood. However, for some reason, my body was not accepting the A+ blood and they noticed that my levels were not changing. They ran several tests but could not figure out the problem.
After sending my blood to a specialist I was told that I have to receive A+ blood with a capital A antigen at a certain place in the chart the doctor gave me (on the 13th spot if I remember correctly. No worries I have given copies to all my medical professionals just in case).
I have searched for other instances for this but nowhere have I found anything similar. It was made very clear to me that this is something I need to make sure I give my medical professionals if I ever have surgeries but it always seems to stump some of them.
I was just wondering If you have ever heard of this before. I can never find information on it and want to know more. I always read about the RH stuff but none of it even covers what I was told and I never see references to a Capital A antigen.
Maggie, it’s not completely clear what you are describing to me, and I really can’t do medical consultation through the site anyway. The most important thing is that those records you mention are known to those taking care of you. I’m sorry I can’t help you more, but the terminology can be confusing, and seeing exactly what is written is the only way to be sure. I wish you the very best.
-Joe
Hi Joe:
Have ever experienced a different in the reaction strength of Anti-c (little c) and Anti E (big E) with R2R2 vs rr. We are seeing +2 reactivity with rr and negative with R2R2.
we know that R2R2 had the highest number of D antigens.
Thanks
Hi there,
Just want a bit of understanding of my supposedly strange blood combination when in comparison to my ethnicity.
I’m Lithuanian (WHITE), both parents Lithuanian. However, my blood is B+ (most common amongst Asian) with a positive R0 Subtype (most commonly found in African Americans).
Any idea what I could research to find out a bit more? Thanks.
Ps I’m aware that Lithuanian tribes emerged from Indo/Europe/
Thanks.
Ed
Hi Joe,
I am currently reviewing for my SBB and what would the probability of having an Rh negative kid if there are more than 8 offspings? I’m just curious because the Punnet square only show like the probability to just 4 children. What if there are more? Can you help me understand like how to do the inheritance pattern for mom that has more than 6 or 8 children? Thank you!
Cath, the possibilities there are the only possibilities from those two parents, no matter how many kids there are in the family (by simple Mendelian genetics, anyway). In that example, each child born, whether they are the first-born or the eight-born or the eleventh-born, has a 50% chance of being R1r and a 50% chance of being R0r.
-Joe
Hi Joe, I’m in SBB school rn and usually when we want to calculate the 6th or 8th child you multiply the % 6 times or 8 times to figure out the chance of having that ag. In this case it would be (.50)(.50)(.50)(.50)(.50)(.50) etc.. the 6th child or 8 x for the 8th child… correct me if I’m off 🙂
At risk of sounding very ignorant, what does it mean by R1wR1? How does it differ from R1R1?
Can you tell me more specific my blood type Type B Rh DCE Neg
Hi, I am trying to understand this better but I guess I can’t. I am a regular blood donor and I went to donate my blood this morning. The nurse told me that my phenotype R1RZ. I didn’t understand that but she said that my blood type is suitable for the Thalasemia patients.
Appreciate if you could explain further on this, in a layman term. I am a potential kidney donor for my daughter. She is a CKD stage 5 patient and she is O. The difference of our blood type will still allow us to do because the crossmatch test done is negative.
However, I still need further explanation from you on this.
Thank you very much.
Hi, Prior to surgery and after a blood test, I was given a card to be carried by person with unusual blood group showing the following:
Cells: Rh (D) pos R1r
Serum: Anti – E
I have been trying to find out my blood group and what the above means.
On occasion I have attempted to donate blood but was always asked “do you have a cold”. Then they would do a test and it would come back that all was well. I really don’t understand and my GP is probably not the person to advise. Can you help?
I know nothing about blood, but my late mother worked at a regional blood bank in UK and was a regular blood donor, until they found her blood had a particular factor – R2R2 – and they asked her not to donate unless called for. One day a taxi arrived at our house to whisk her off to give blood for Simon Bostick, the bone marrow transplant baby. I just wondered what the import of R2R2 is, whether I might have inherited it and, in that case, whether my blood (O-pos, like hers) might be useful to someone. I have donated blood but mine has not been tested for R2R2.
Greeting
Is there a table for rh phenotype compatiblity match? i.e compatiblity between different rh phenotype suppose ABO and D are same.
Why is it Doctors can’t explain things how they should.
Here it is in simple terms
Over 50 percent of the population is Heterogeneos for Blood type and pheno type and also RH factor. AO +- and BO +-together these two types can make any of the blood groups positive r negative and the reason it’s so important is if it wasn’t like this before rohgham it would have drastically effected the population growth as they had no idea of the incompatibility but a doctor will never admit that.
Greetings
is there any cheat sheet for Rh compatibility that we can depend on it (i.e R1r with R1R1 matching) of the same ABO blood group?
Revo
Hi Joe,
Love your show
Anyway you can explain the different RHD and RHCE variants 🙂 I can’t wrap my brain around them…..
Thanks
I’m blood type A- and after donating blood in college, i was told.
I had a full term pregnancy later, and when I went to donate blood at the Red Cross, I received a card saying they couldn’t take my blood because I had an antigen or antibody, I forgot which.
So why can’t I donate blood anymore?
Sorry, MJ, theres really no way for me to tell without knowing more of your history. I’d suggest you check with your local Red Cross donor center, if one is near you, as they should be able to find out the reason. Chances are it was an antibody, but there’s no way to tell which one without more detail. I wish you the best!
-Joe